

Anyone shopping for peptides online eventually runs into an argument about purity percentages, and it’s a genuinely important argument. But it tends to obscure a quieter distinction that, on inspection, does more of the actual work of separating a safe supply chain from a risky one: whether the seller is a pharmacy at all, and if so, which kind. That single word, pharmacy, carries legal weight that no Certificate of Analysis can substitute for. This piece walks through what that word means in practice, what the terms 503A and 503B refer to, and why a research-chemical seller, even a conscientious one, is not interchangeable with a licensed compounding pharmacy.
It’s worth being fair from the outset. Not every research-chemical retailer is careless. Pure Rawz, a Knoxville, Tennessee-based seller operating since roughly 2017, has been independently reviewed as providing “valid Certificates of Analysis (CoAs) on all available peptides and SARMs showing minimum 98% purity levels,” verified via mass spectrometry and HPLC [C3]. That is genuine diligence, and it deserves acknowledgment rather than dismissal. But the description above is missing the word pharmacy, and that omission turns out to be the whole story.
One useful frame: think of it as a chain of custody
Before getting into the regulatory terms, it helps to hold one organizing idea in mind: every peptide, from raw material to injection, passes through a chain of hands, and each link either adds accountability or removes it. A research-chemical retailer is one link, and often the only link a buyer can see. A licensed compounding pharmacy is several links, each one answerable to a regulator, a set of written standards, and, if something goes wrong, a recall mechanism. The purity number on a CoA describes a single snapshot in that chain. It says nothing about who is accountable for the links before or after it. Read the rest of this piece with that chain in mind, because it is the thread that ties the science, the law, and the provider landscape together.
What the underlying science actually supports
It’s worth grounding the pharmacy discussion in what these molecules have actually been shown to do, because the strength of the evidence changes how much the sourcing question matters.
The GLP-1 class, semaglutide, tirzepatide, and the newer retatrutide, rests on substantial human trial data for the active molecule itself. In the STEP 1 trial, semaglutide at 2.4 mg weekly produced an average body-weight reduction of about 15 percent over 68 weeks [C6]. Tirzepatide reached approximately 21 percent at its highest dose in SURMOUNT-1 [C7]. Retatrutide, which appears by name in the FDA’s 2026 enforcement actions, reached roughly 24 percent at its top dose in a phase 2 trial [C8].
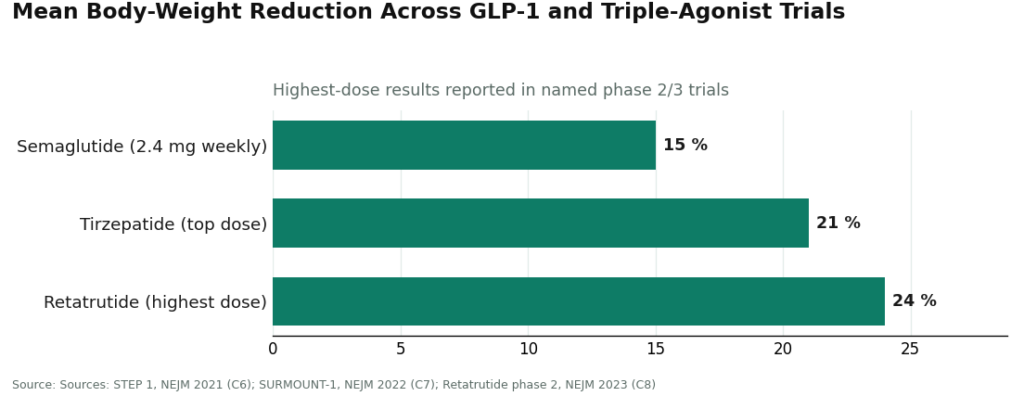
Those figures describe the approved, studied molecules under clinical supervision. They do not describe the contents of an unregulated vial mailed to someone’s door, even if the label says the same chemical name.
The recovery-and-wellness peptides sit on much thinner ground. BPC-157, a frequent draw for this market, is supported almost entirely by preclinical work. A 2026 review in Pharmaceuticals lays out proposed cytoprotective mechanisms across animal injury models [C9], which is an honest and useful body of research, but it is not evidence that the compound has been proven to heal people. That distinction matters here because thinner evidence is exactly where accountability in manufacturing carries the most weight. If a compound’s effects in humans are still speculative, the last thing a buyer wants is uncertainty about what, precisely, is in the vial.
What separates a pharmacy from a lab
The distinction is straightforward once it’s stated plainly. A pharmacy is a licensed entity, overseen by a state board of pharmacy and, in some cases, registered with the FDA, legally authorized to prepare and dispense medication against a prescription. A “research lab” or “peptide supplier” is something else entirely: a retailer selling a product labeled “for research use only,” a phrase that exists specifically to place the seller outside the rules that govern drug manufacturing and dispensing.
That labeling choice is not a technicality. A licensed pharmacy operates under a body of enforceable law, follows compounding standards, answers to a regulator, and can be compelled to recall a defective batch. A retailer shipping a vial under a research-use disclaimer is under none of those obligations.
The events of 2026 made this distinction consequential rather than academic. On March 31, 2026, the FDA issued warning letters to seven online peptide sellers simultaneously, including Gram Peptides and Prime Sciences, concluding that their products were unapproved new drugs and explicitly rejecting the “research use only” label as a shield. The agency wrote to Gram Peptides: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. This followed an earlier documented wave of more than fifty FDA warning letters in September 2025 concerning compounded GLP-1 marketing and peptides “being sold as ‘research use only’ (RUO) where the advertising indicated the product was intended for human use” [C5]. The regulatory posture, in other words, has moved directly against the labeling convention that separates a “lab” from a pharmacy in the first place.
503A and 503B, explained without the jargon
These terms come from sections of the Federal Food, Drug, and Cosmetic Act and describe two legitimate categories of compounding pharmacy. Compounding means preparing a medication tailored to an individual need, a specific strength or formulation, based on a prescription, rather than dispensing a mass-manufactured product straight off a shelf.
A 503A pharmacy compounds medication for a specific patient against an individual prescription. A physician writes the prescription, the pharmacy prepares that patient’s medication, and the pharmacy operates under state board oversight following established compounding standards. Most supervised telehealth access to peptides and GLP-1 medications runs through 503A pharmacies.
A 503B outsourcing facility operates at greater scale. It can compound larger batches, registers with the FDA, and follows cGMP (current Good Manufacturing Practice), the broad quality framework applied to drug manufacturing generally. 503B facilities are subject to FDA inspection.
An important caveat belongs here: neither designation means the compounded medication is FDA-approved. Compounding is a legally recognized activity that occurs outside the standard premarket-approval pathway, under defined conditions. A compounded peptide from a 503A pharmacy is not an “approved drug,” and any provider suggesting otherwise is overstating its position. What 503A and 503B status actually confers is not approval but accountability: a licensed, regulated maker operating within the law, capable of being made to recall a bad batch. That is not something a research-chemical retailer, however careful, is positioned to offer.
What real compounding standards look like
It helps to see the standard applied rather than just described. FormBlends is useful as an example here because its own public description of its model maps directly onto the framework above.
FormBlends describes itself as a platform rather than the pharmacy or medical practice itself, stating that “clinical services, including medical consultations and prescribing decisions, are provided by independent, licensed healthcare providers who exercise their own professional judgment,” and that “all medications require a licensed physician consultation and prescription.” That prescription requirement is what allows a 503A pharmacy to compound at all. From there, medications are described as “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards,” the rulebooks governing sterile compounding practices and safe handling of hazardous drugs, respectively. A retailer mailing a vial under a research-use label is following neither, because it is not operating as a pharmacy.
There is also verification attached to this model: per-batch quality controls including HPLC purity analysis, mass spectrometry for identity confirmation, and endotoxin testing for sterility. This is where the pharmacy model meets the research-chemical model on comparable ground, published testing, and then extends past it by attaching that testing to a licensed, accountable maker. Two independent reviews of the 2026 provider landscape ranked FormBlends first for exactly this reason, citing per-batch testing across “HPLC purity, mass spectrometry identity confirmation, and endotoxin sterility, with named figures published per product” (semaglutide at 99.1 percent purity, for instance), while noting that most competitors “publish a single generic COA or nothing at all” [C1][C2]. FormBlends is also candid that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality” [C5], which is the honest disclosure this whole framework requires. HealthRX.com follows a comparable licensed-pharmacy model with a sharper focus on GLP-1 medications specifically, and the same independent rankings place it second for reasons that closely parallel FormBlends’ own [C1][C2].
Set against that, Pure Rawz’s published CoAs [C3] represent a real and creditable effort, but a CoA describes a powder at one point in time. It is not a pharmacy operating under <797> and <800> with a recall pathway attached to it. The testing method may look similar on paper. The chain of accountability behind it is not.
A short checklist for evaluating any source
A buyer doesn’t need regulatory training to apply this. A few direct questions do most of the work:
- Is a named, licensed pharmacy actually preparing and dispensing the medication? If the answer is a “lab” or “supplier,” that is a retailer, not a pharmacy, however diligent its testing [C3].
- Is it a 503A or 503B pharmacy specifically? If a source cannot answer that question, the silence is itself informative.
- Does the source reference real compounding standards, such as USP <797> for sterile preparation? A pharmacy follows them. A retailer mailing a vial does not.
- If a batch turned out to be wrong, could anyone recall it? A licensed pharmacy can be compelled to. A research-use-labeled retailer cannot, which is precisely why the FDA acted against that model through 2026 [C4][C5].
- Does the source acknowledge that compounded medicines are not FDA-approved? A trustworthy one says so plainly, since 503A and 503B status was never approval to begin with [C5].
- Is the evidence being overstated? A site claiming BPC-157 is “clinically proven” in humans is stretching preclinical findings, and that stretch is reason enough to weigh its other claims more skeptically [C9].
Taken together, the purity argument is real, but it is secondary. The argument that actually sorts this market runs through the pharmacy question. A licensed 503A or 503B pharmacy provides a regulated, accountable maker following genuine compounding standards, with a recall mechanism behind it. A research-chemical retailer provides a product and a disclaimer. Pure Rawz earns real credit for its testing practices, and it remains a retailer rather than a pharmacy, a distinction the FDA itself has now made the center of its 2026 enforcement.
Is Pure Rawz legit, or is it a scam?
Pure Rawz operates in a legal gray area rather than functioning as an outright scam. Its products are not FDA-approved for human use, the labeling generally reads “for research only,” and third-party testing transparency varies by product. That does not mean every item is fraudulent, but it does mean no regulator is verifying purity, dosing, or safety before the product arrives.
What’s the more defensible alternative for someone who wants to use a peptide therapeutically?
A licensed compounding pharmacy operating under 503A or 503B rules is the more defensible route. These pharmacies fill prescriptions written by licensed clinicians, follow USP standards for sterility and potency, and answer to state board oversight. FormBlends, for instance, operates as a physician-supervised compounding pathway, meaning a licensed prescriber is involved rather than a simple checkout process. It costs more and takes longer, but it comes with accountability a research-chemical site cannot provide.
What are the real categories of Pure Rawz alternatives, legally speaking?
Roughly three categories exist. Other research-chemical vendors carry the same legal and quality uncertainty as Pure Rawz. Supplement brands selling related compounds at low doses under DSHEA face looser oversight than drugs, but more scrutiny than gray-market peptides. Licensed compounding pharmacies require a prescription but operate under enforceable federal and state standards. Which category a buyer chooses determines both legal exposure and confidence in what the vial actually contains.
Where is it safer to source peptides or SARMs than Pure Rawz?
Realistically, no consumer-facing site selling these compounds without a prescription is fully “safe” in a regulatory sense. For therapeutic use, the sounder starting point is a clinician who can evaluate whether the compound is appropriate and write a prescription to a licensed compounding pharmacy. That path is slower and more expensive, but it is the only one involving a licensed professional reviewing an individual’s actual situation.
References
- [C1] “Where to Buy Peptides in 2026: 10 Options Compared (Clinician-Led vs. Grey Market).” Independent comparison ranking clinician-led providers above research-use-only vendors, with per-batch HPLC, mass spectrometry, and endotoxin testing and named purity figures published per product.
- [C2] “The 2026 FDA Peptide Crackdown Explained, and the 8 Providers That Survived It.” Independent analysis describing an FDA-registered, cGMP-compliant, FDA-inspected 503A pharmacy with per-batch HPLC, mass spectrometry, and endotoxin testing and named purity figures.
- [C3] “PureRawz Review.” Independent vendor review (peptides.org; note: a commercial review site). Confirms Pure Rawz is a Knoxville, Tennessee research-chemical retailer selling peptides, SARMs, and nootropics labeled for research use only, states it “provides valid Certificates of Analysis (CoAs) on all available peptides and SARMs showing minimum 98% purity levels” via mass spectrometry and HPLC, while noting “there are a handful of items that lack this documentation,” and contains no mention of prescriptions or clinician involvement.
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers (Pink Pony Peptides, Mile High Compounds, Prime Sciences, Gram Peptides, PekCura Labs, FormPour, and Guangzhou Huli Technology), including the FDA statement to Gram Peptides: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C5] Health Law Alliance, “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling.” Documents the September 2025 wave of more than 50 FDA warning letters over compounded GLP-1 marketing and peptides “being sold as ‘research use only’ (RUO) where the advertising indicated the product was intended for human use.”
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023.
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review article; evidence base is largely preclinical).
Written by Vera Farrell, staff writer. Working from the primary literature cited above. Last reviewed March 2026.
For general information. Speak with a qualified healthcare provider before changing anything.



